|
|
|
|
Araştırma Makalesi Research Article |
İmmünoloji Laboratuvarında
Akılcı Test Seçimi: Antinükleer Antikor (ANA) İstemlerinin ve Sonuçlarının Diğer
Testler ile Birlikte İncelenmesi Choosing Wisely in Immunology
Laboratory: Reviewing of Antinuclear Antibody (ANA) Test Requests and Results
Together with Other Tests *Kemal TEKİN1
[ID], Hasan
KARAKUŞ1 [ID], Sevinç
KARABULUT1 [ID], Fatih
ŞAHİNER2 [ID], Özet Bu çalışmada bir üçüncü basamak
eğitim ve araştırma hastanesinin tıbbi immünoloji laboratuvarında çalışılan
testlerin dağılımını ve pozitiflik oranlarını incelemek ve iş yükünün önemli
bir bölümünü oluşturan antinükleer
antikor (ANA) testi istemlerinin hastalık tanı/ön tanılarına ve klinik
birimlere göre dağılımını belirlemek,
hatalı-uygunsuz test istemlerinin olası
nedenlerini ve maliyetini incelemek ve etkin ve uygulanabilir çözüm önerilerini ele almak amaçlanmıştır. Çalışmada, Eylül 2016 tarihinden itibaren yaklaşık üç yıllık bir dönemde çalışılan tüm immünoseroloji
testlerine (n=94.954 ayrı parametre)
ait verilerin retrospektif bir incelemesi sunulmuştur. Testler üç ana gruba ayrılarak ele alındığında; tüm test parametreleri arasında %20.3’lük (n=19.248) bir oran ile ilk sırada ANA testleri yer almaktadır. Çalışmamızda indirekt
immünfloresan antikor (IFA) yöntemi ile
değerlendirilen ANA testlerinin pozitiflik oranı %23.1 (n=4446) olarak
bulundu. Çok sayıda farklı testi içeren (IFA, ELISA ve immunoblot temelli)
spesifik otoantikor testlerinin raporlanan parametre sayısı ise 67.976
olup ikinci grupta yer alan bu testlerin genel pozitiflik oranı %2.96 idi ve antikor tipine göre %0.8 ve %12.7 arasında değişmekte idi. Üçüncü grupta yer alan ELISA temelli
brusella ve antiviral (herpes simplex virus 1 ve 2, varicella virus, measles
virus, mumps virus, parvovirus B19) IgM ve IgG
antikor testlerinde ise istenilen test sayısına göre en yüksek pozitiflik
oranı (%30.1, 2324/7730) gözlemlendi.
ANA pozitif hastalarda ANA ile ilişkili otoantikorlardan en sık
saptananlar anti-dsDNA (%9.2) ve anti-SS-A (%8.2) olarak bulundu. Eş zamanlı
test istemi yapılan ANA ilişkili otoantikorlar için, ANA negatif hastalarda anti-dsDNA
pozitifliği %3.3 olarak bulunurken, ANA
ilişkili diğer spesifik
otoantikorlar için
pozitiflik oranları %0.0-0.31
aralığında değişmekte idi. ANA testleri için en çok istem
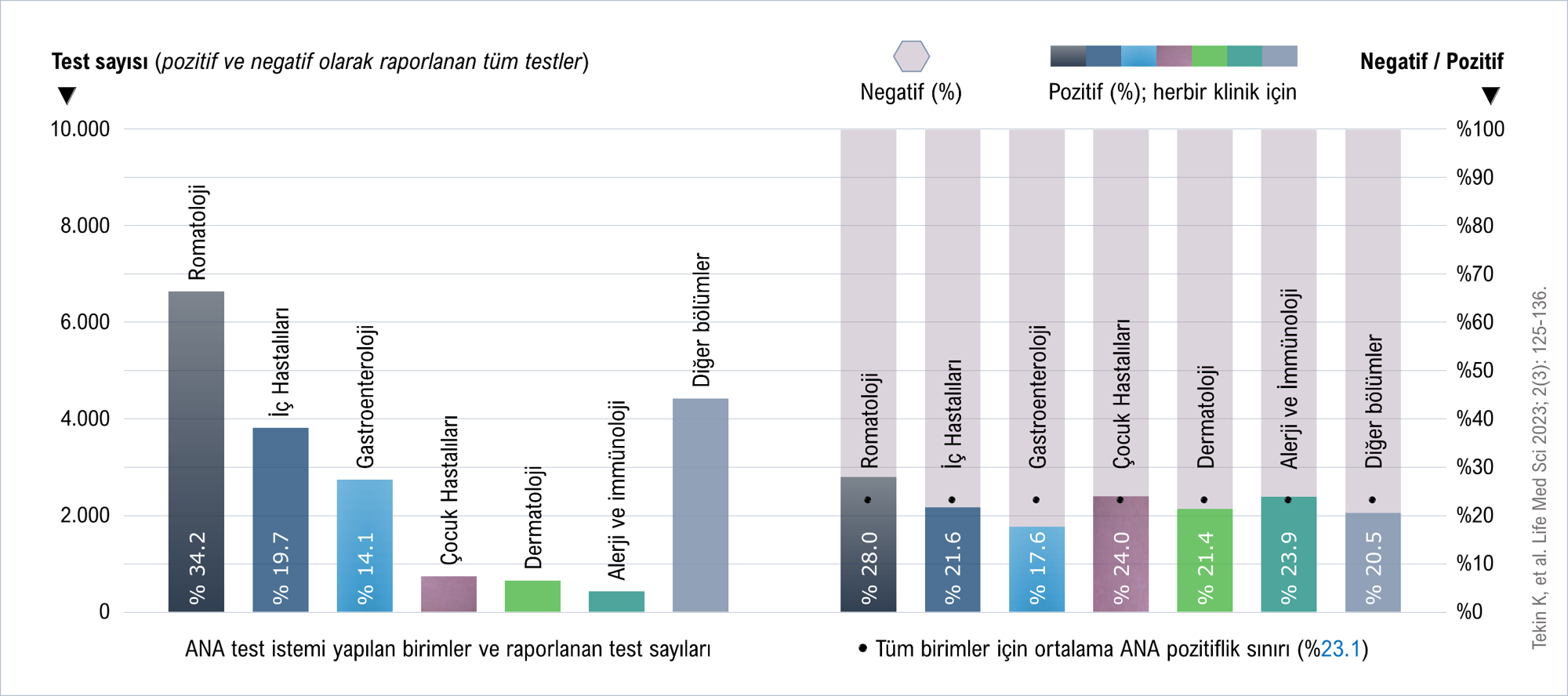
yapılan (%34.2) ve en yüksek ANA pozitiflik oranının (%28) görüldüğü birim romatoloji idi. Gereksiz test istemi
nedenleri arasında en
dikkat çekeni, aynı hasta için farklı hekimlerin yaptıkları test
istemleri idi. ANA testlerinin 1:100 dilüsyonda çalışılmasının düşük pozitif
sonuçlar nedeni ile gereksiz ikinci basamak test (spesifik otoantikor) çalışılmasına neden olabileceğini ve dar kapsamlı ikinci basamak otoantikor test
panellerinin laboratuvar verimliliği üzerine olumsuz etkileri olacağını
değerlendirmekteyiz. Anahtar kelimeler: Antinükleer
antikor, ANA, İmmünoloji, Maliyet etkinlik. Abstract In this study, it
was aimed to examine the distribution and positivity rates of the tests
reported in the medical immunology laboratory of a tertiary education and
research hospital, and to determine the distribution of antinuclear antibody
(ANA) test requests, which constitute a significant part of the workload,
according to disease diagnosis/preliminary diagnoses and clinical
departments, and to examine the possible causes and costs of
incorrect-inappropriate test orders, and to consider effective and applicable
solution suggestions. In the study, a retrospective review of data on all immunoserology tests (n=94,954 individual parameters)
reported approximately over a three-year period starting from September 2016
was presented. When the tests are divided into three main groups; among all
test parameters, ANA tests ranked first with a rate of 20.3% (n=19,248). In
our study, the positivity rate of ANA tests evaluated by the indirect
immunofluorescence antibody (IFA) method was found as 23.1% (n=4,446). The number
of reported parameters of specific autoantibody tests (second group), which
include many different tests (IFA, ELISA, and immunoblot based), was 67,976,
and the overall positivity was 2.96%, varies between 0.8% and 12.7%,
depending on the antibody type. In the ELISA-based brucella and antiviral
(herpes simplex virus 1 and 2, varicella virus, measles virus, mumps virus,
parvovirus B19) IgM and IgG antibody tests in the third group, the highest
positivity rate was observed according to the number of tests requested
(30.1%, 2,324/7,730). In ANA-positive patients, the most frequently detected
ANA-related autoantibodies were anti-dsDNA (9.2%) and anti-SS-A (8.2%). In
ANA-negative patients, in simultaneously ordered tests, anti-dsDNA positivity
was found to be 3.3%, while positivity rates for other ANA-related specific
autoantibodies were in the range of 0.0-0.31%. ANA tests were most frequently
ordered from the rheumatology department (34.2%), and also the highest ANA
positivity rate (28%) was observed in this unit. The most notable reason for
unnecessary test ordering was the test requests by different physicians for
the same patient. We consider that evaluation of ANA tests at a dilution of
1:100 may lead to unnecessary second-step testing (specific autoantibodies)
due to the low positive results, and that narrow-scope second-step
autoantibody test panels will have negative effects on laboratory efficiency. Keywords: Antinuclear antibody, ANA, Immunology,
Cost effectiveness.
Şekil 1. ANA test istemlerinin (raporlanan)
kliniklere göre dağılımı ve pozitiflik oranları. Şekil 1 png Figure 1. Distribution of
ANA test orders (reported) by clinics and positivity rates. Figure 1 png
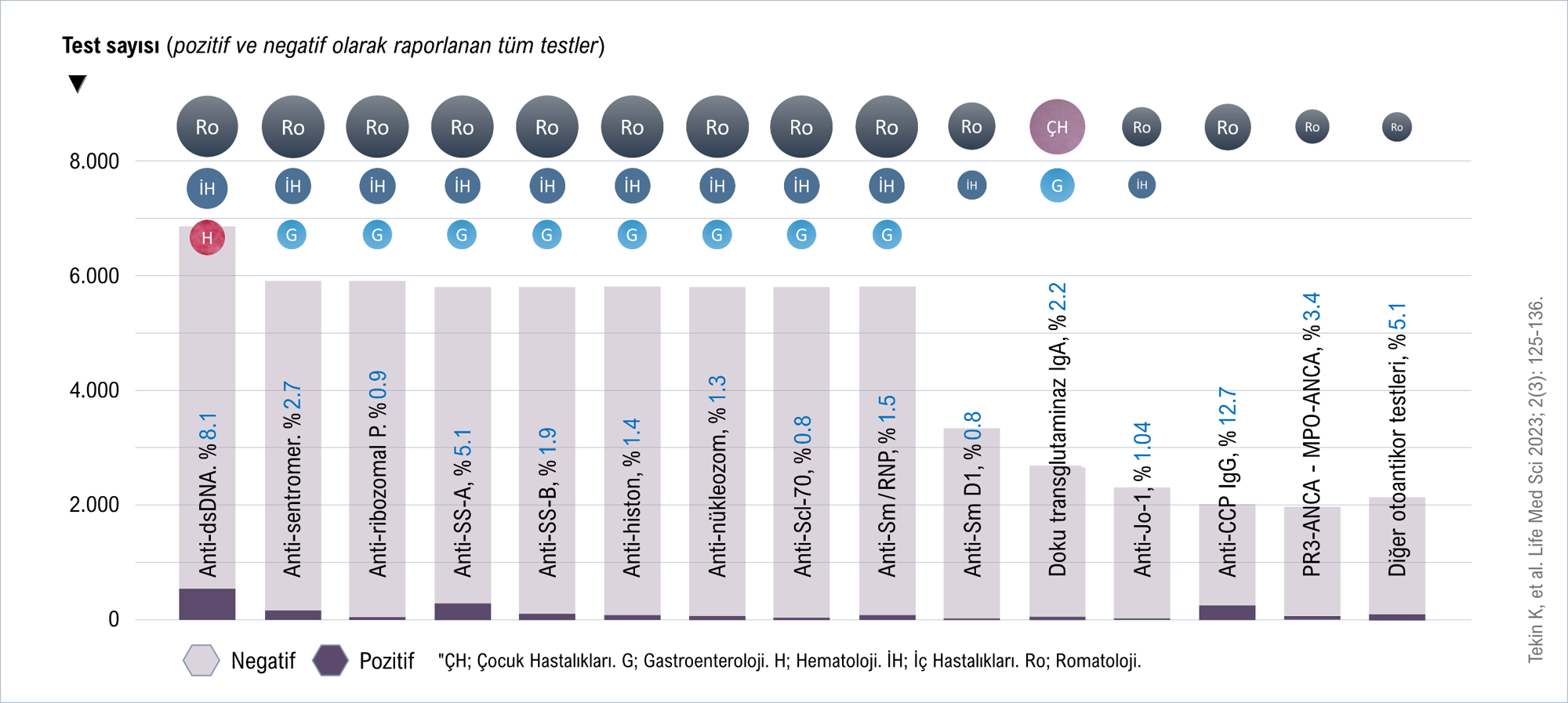
Şekil 1. İmmünoseroloji laboratuvarında
çalışılan ANA dışındaki diğer testler ve pozitiflik oranları (%). Sütunların
koyu renkli bölümleri pozitif, açık renkli bölümleri ise negatif test sayılarını temsil etmektedir. Şekil 2 png Figure 1. Tests other
than ANA studied in the immunoserology laboratory
and positivity rates (%). The dark-colored parts of the columns represent
positive test numbers, and the light-colored parts represent negative test
numbers. Figure 2 png |
|
DOI: 10.54584/lms.2023.38 |
|
|
Article in Turkish |
|
|
|
|
|
|
|
|
1Medical Microbiology Laboratory,
Gulhane Training and Research Hospital, University of Health Sciences,
Ankara, Türkiye. 2Department of Medical Microbiology,
Gulhane Medical Faculty, University of Health Sciences, Ankara, Türkiye. |
|
|
|
|
|
*Corresponding author Kemal Tekin, MD., Medical Microbiology
Laboratory, Gulhane Training and Research Hospital, University of Health
Sciences, Ankara, Türkiye. E-mail: ktekin1978@gmail.com |
|
|
|
|
|
Received: 10.06.2023 Accepted: 14.07.2023 Published: 16.07.2023 |
|
|
Cite as: Tekin
K, Karakuş H, Karabulut S, Şahiner F, Gümral R. Choosing Wisely in Immunology
Laboratory: Reviewing of Antinuclear Antibody (ANA) Test Requests and Results
Together with Other Tests. Life Med Sci 2023; 2(3): 125-136. |
|
|
|
|
|
View in academic indexes and databases |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cited by 1 article*, 0 book chapter. |
|
|
[1]* Aygar İS, Cebeci İ. Five-Year Analysis of Anti-Nuclear
Antibody (ANA) and Extractable Nuclear Antigen Antibody (anti-ENA) Immunoblot
Test Results. Life Med Sci 2023; 2(4): 143-149. doi: 10.54584/lms.2023.40 |
|
|
©Copyright LMS.
Licensed by Creative Commons Attribution-NonCommercial 4.0 International (CC
BY-NC 4.0). |
|